
This week we made it all the way up to the head. To look at the anatomy of the head, we need to start by looking at the bones. Different stations looked at different parts of the skull and teeth, and I spoke about the temporal region.
The temporal region (or as laymen may call it, your “temples”) lies superior to the zygomatic arch and within the edges of the temporalis muscle. You may see curves on the skull around the edge of the temporal fossa that correspond to the attachment of the flat temporalis muscle. There is a depression here in which a few superficial structures lie, and this is the temporal fossa.
 The bones here are the parietal bone, the temporal bone (it has squamous – flattened – and petrous – lumpy/rocky – parts) and the sphenoid bone. Use the skull bone images here to see these. Note also the frontal bone and the zygomatic bone. Spend some time in the lab with a coloured skull and a detailed skull (the numbered ones are best) to be clear on the shapes of these bones.
The bones here are the parietal bone, the temporal bone (it has squamous – flattened – and petrous – lumpy/rocky – parts) and the sphenoid bone. Use the skull bone images here to see these. Note also the frontal bone and the zygomatic bone. Spend some time in the lab with a coloured skull and a detailed skull (the numbered ones are best) to be clear on the shapes of these bones.
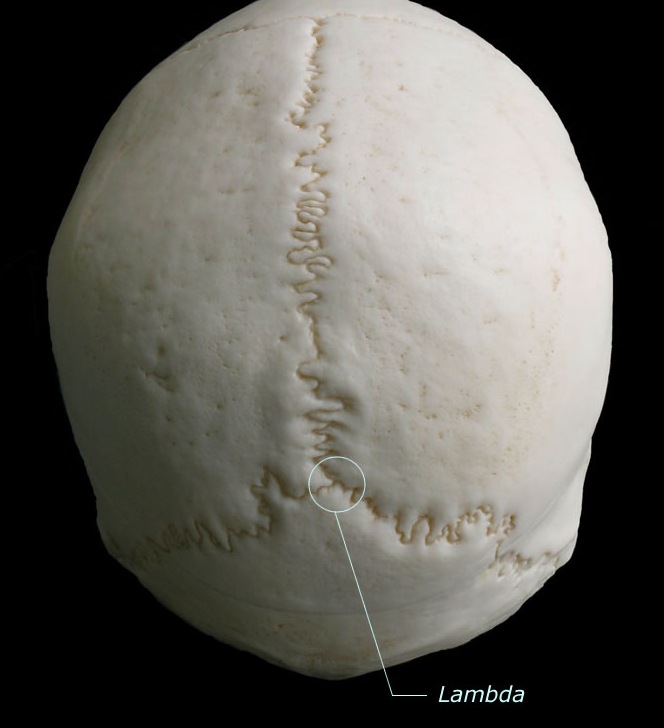
We talked about the nature of sutures linking the bones of the skull, which are fixed in the adult and contribute to the aim of the skull to protect the brain. There are some sutures that you should be able to name and you can also see these in the skull images (here). Note also the bregma (where the coronal suture meets the sagittal suture) and the lambda (where the sagittal suture meets the lambdoid suture).
These points correspond to where the anterior and posterior fontanelles were at birth. The bones of the skull are able to slide over one another to some extent to aid passage through the birth canal, and this is known as moulding. The bones are not fixed by sutures at this time, but are linked by softer membrane-like connective tissues. After birth the anterior fontanelle is known as the soft spot and can be an important diagnostic indicator. The fontanelles also allow the bones of the skull to grow.
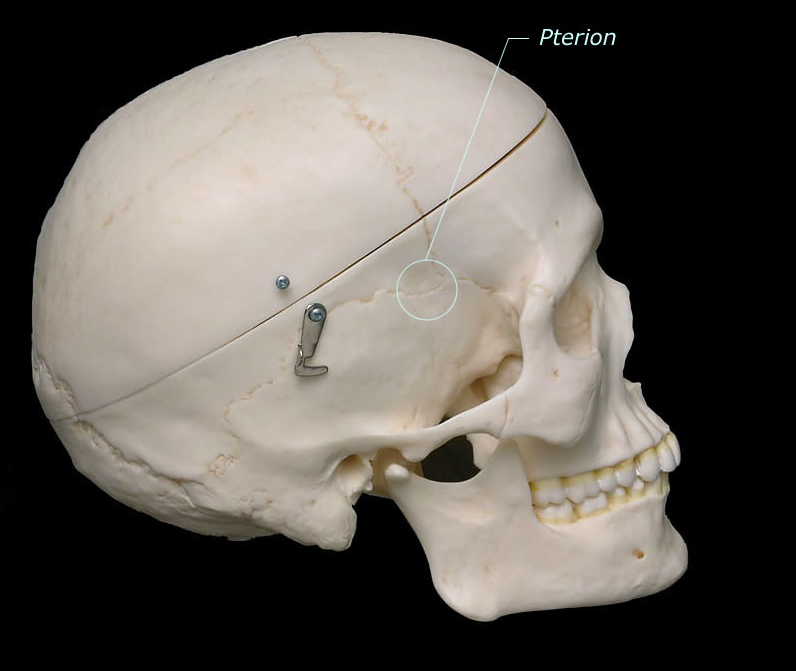 Back to the temporal region: the sutures linking the parietal, frontal, sphenoid, and temporal (squamous) bones join here to form an H-shaped group of sutures known as the pterion. This potential weakness in the skull is made weaker by a thinning of the bones here (you can often see this on real skulls in the lab, but not on plastic skulls). To make matters even worse, the middle meningeal artery runs inside the skull, deep to the pterion. A fracture here is likely to tear the middle meningeal artery, causing blood to pool between the bone and the dura mater, pressing on the brain. This is an extradural haemorrhage and can be fatal (and in fact, dural venous sinuses may also be involved).
Back to the temporal region: the sutures linking the parietal, frontal, sphenoid, and temporal (squamous) bones join here to form an H-shaped group of sutures known as the pterion. This potential weakness in the skull is made weaker by a thinning of the bones here (you can often see this on real skulls in the lab, but not on plastic skulls). To make matters even worse, the middle meningeal artery runs inside the skull, deep to the pterion. A fracture here is likely to tear the middle meningeal artery, causing blood to pool between the bone and the dura mater, pressing on the brain. This is an extradural haemorrhage and can be fatal (and in fact, dural venous sinuses may also be involved).
The temporal fossa has a few superficial structures of interest passing through it. The pulse you feel in your “temples” is the pulse of the superficial temporal artery, a branch from the end of the external carotid artery. The superficial temporal vein, draining a similar area of the scalp, is nearby. The superficial nerve here is the auriculotemporal nerve. This nerve carries sensory information from this area, and is a branch of the mandibular nerve, which itself is a branch of the trigeminal nerve, also known as cranial nerve V (CN V). I have a feeling we will be meeting this nerve again in the future when we start adding more detail to our head and neck anatomy and look at the infratemporal fossa. For example, this nerve also carries parasympathetic nerve fibres from CN IX to the parotid gland (that tell it to secrete saliva).
Fun, eh? The anatomy of the head and neck can be very detailed, delicate and intricate. It’s a fascinating region anatomically, and by building up your knowledge bit by bit over the next 18 months or so you should develop a solid understanding of what’s going on in there.